آخر المواضيع المضافة

 النبات
الحيوان
الأحياء المجهرية
علم الأمراض
التقانة الإحيائية
التقنية الحيوية المكروبية
التقنية الحياتية النانوية
علم الأجنة
الأحياء الجزيئي
علم وظائف الأعضاء
الغدد
المضادات الحيوية
النبات
الحيوان
الأحياء المجهرية
علم الأمراض
التقانة الإحيائية
التقنية الحيوية المكروبية
التقنية الحياتية النانوية
علم الأجنة
الأحياء الجزيئي
علم وظائف الأعضاء
الغدد
المضادات الحيوية| Polygenic and Multifactorial Inheritance |


|
|
Read More
Date: 30-10-2015
Date: 10-11-2015
Date: 11-11-2015
|
Polygenic and Multifactorial Inheritance
INTRODUCTION
There are many disorders, which have familial clustering, but do not follow a Mendelian pattern of inheritance. Many common congenital malformations and some diseases of adulthood fall into this group. Family studies show more than one family member or near relative affected with a disorder but their percentage is much lower than single gene disorders. The underlying cause is not known but it is believed that many genes are responsible, which can get triggered by environmental factors. These gene loci each act in an additive fashion, and no one gene is responsible.
An inheritance is called polygenic, when many genes present at different loci, with each gene having some additive effect, control a trait. In a multifactorial disorder, both genetic and environmental factors contribute, where genetic contribution is from both the parents. Thus genes and environmental factors as multifactorial traits can vary in different individuals.
QUANTITATIVE AND QUALITATIVE TRAITS
Quantitative traits are measurable, and some examples are serum cholesterol, height and weight. This means there exists an unlimited value between the upper and lower limits of a value, which has definite range. In qualitative traits, the phenotypes are either present or absent. An example of this is achondroplasia. The inheritance pattern in quantitative phenotypes (normal variation) is inherited as a multifactorial trait.
Normal Variation
The majority of phenotypic differences among normal persons are due to multifactorial traits, for example height, intelligence, and skin colour. In normal quantitative traits a child’s phenotype is normally the average of his parents’ value, which is often referred to as a midpoint value.
Linkage Studies
Linkage studies are of great value in identifying contributory genes by molecular methods. They are useful in identifying underlying causes in multifactorial diseases.
Characteristics of Multifactorial Disorders
a- Diseases appear familial, but there is no monogenic pattern.
b- Frequency is higher in one sex than in the other. Examples include pyloric stenosis, which is more common in males, while systemic lupus erythematosis (SLE) is more common in females.
c- Recurrence risk is same for all the relatives. It is dropped when relationship is more remote.
d- Recurrence risk in multifactorial inheritance is lower in a population where incidence is lower.
The normal incidence of multifactorial disorders is 1 in 1000. The recurrence risk in siblings or children of affected is 2-4%. Multifactorial diseases of adult origin have a 1% population risk. The risk to siblings and children is 5 - 10%. Multifactorial diseases are more common in the progeny of consanguineous marriages as their genetic pool contains similar abnormal genes.
FACTORS INFLUENCING RECURRENCE RISK
Familial Clustering
The recurrence risk is increased if more than one near relative is affected, as well as if more than one child is affected. This is different from monogenic inheritance, where recurrence risk is totally dependant on parental genotypes, and is independent of previously affected children.
Recurrence risk is higher if a proband is more severely affected. The recurrence risk is also higher in relatives of an affected person, if the sex involved is less frequently associated with the disease. For example, if an affected child with pyloric stenosis is male, the recurrence risk to his brother is 3-8% and 9.2% if the affected child is female. These examples are different from monogenic and chromosomal disorders, where severity of the disorder in the proband does not affect the recurrence risk.
The Diagnosis is Always Made by Exclusion
Isolated cleft lip and cleft palate individually or in combination exhibits multifactorial inheritance, may be part of a chromosomal syndrome, or may occur due to teratogenic factors. Spina bifida is another condition, which is mostly inherited as a multifactorial disorder but could be associated with a chromosomal disorder.
As multifactorial diseases are caused by a combination of genes and environment, environmental factors have a great effect when genetic predisposition factors prevail. Prevention of this is possible. An example of this is use of periconceptional folic acid in the prevention of neural tube defects.
Studies in twins are often used to distinguish between multifactorial traits, Mendelian traits or nongenetic factors.
SOME COMMON MULTIFACTORIAL DISORDERS
These could be categorized into two groups on the basis of the age of onset, in adulthood or those that present at birth (Table 1). The groups of disorders characteristically present at birth or early childhood are: anencephaly and neural tube defects, pyloric stenosis, cleft lip and cleft palate and congenital heart defects. These have been discussed below.
The second group of disorders includes the common chronic conditions that are responsible for morbidity and mortality in adult life. Hypertension, cancer, schizophrenia, coronary artery disease, obesity, and diabetes mellitus. These are discussed on the chapter on genetics of common diseases.
Table1: Common multifactorial disorders

Diseases presenting at birth
Neural Tube Defects
This is the most common congenital malformation seen in clinical practice, comprising mainly of anencephaly and spina bifida and is a leading cause of mortality and morbidity in children, and leads to stillbirth, early infantile death and handicap in surviving children. When it is not part of a syndrome, there is an increased recurrence risk in subsequent pregnancies. Incidence of neural tube defects has a higher distribution pattern in certain geographical areas. For example Sikhs in Britain, Columbia and Canada have twice the overall population rate.
Anencephaly is characterized by the absence of the vault of the skull, the meninges, the forebrain and the overlying skin (Fig. 1 A).
In Spina bifida there is failure of fusion of the arches of the vertebrae typically in the lumbar region, with severity varying from spina bifida occulta where the defect is only in the bony arch, to spina bifida presenting with meningocele and meningomyelocele (Fig. 1 B). Other defects like clubfoot may be associated with NTD.
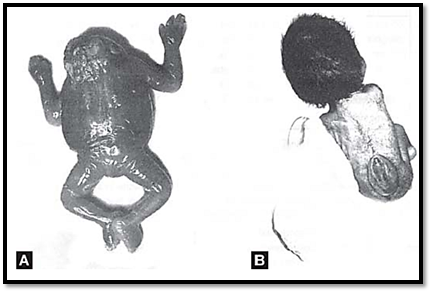
Figs.1A and B: Neural Tube defects (A) Anencephaly: note the absence of skull vault. (B) Spina bifida: meningomyelocele
Pyloric Stenosis
This condition results due to hyperplasia and hypertrophy of the smooth muscles of the pyloric end of the stomach causing narrowing of the antrum of the stomach leading to recurrent obstruction. The male to female ratio per thousand is 1: 5. Increased incidence of pyloric stenosis in males suggests they have a lower liability threshold as compared to the females. Since this condition is surgically correctable, prior consultation with a paediatric surgeon in case of high-risk families during or before pregnancy helps in timely intervention and prevention of complications. Awareness of the existence of the condition and prompt treatment is necessary to avoid lethal complications in the child like aspiration pneumonia.
Congenital Heart Defects
Congenital heart defects have a frequency of 8 per 1000 live births. These form a heterogeneous group of disorders caused by a single gene defects or maternal diseases like rubella infection or diabetes in pregnancy. The incidences of some commonly seen congenital heart diseases are described in Table.2.
Table.2: Incidence of congenital heart defects in normal population
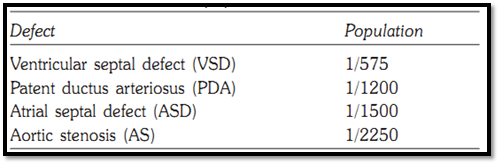
The incidence and relative risk among relatives of the affected sibling decreases with degree of relationship. With high- resolution ultrasound, prenatal diagnosis of major defects is possible by foetal Echocardiography at 18-20 weeks gestation, or slightly earlier at 14-16 weeks with vaginal sonography.
Cleft Lip and Cleft Palate (CL, CP)
One of the most common of congenital malformations, cleft lip and cleft palate result from failure of fusion of the frontal process with the maxillary process at the 35th day of gestation (Fig. 2). 60-80%-affected individuals are males. The causative factor comprises of a heterogeneous group that includes single gene defects, chromosomal disorders (trisomy 13) and teratogenic exposure (rubella embryopathy, thalidomide, and anticonvulsants). The recurrence risk increases with increasing severity. From unilateral to trilateral and from isolated CL to both CL and CP Analysis of population at large with CL (P) reveals that in certain populations there might be a major gene for liability to CL (P) in addition to multiple minor genes.

Fig. 2: Cleft lip with cleft palate
References
Purandarey , H. (2009) . Essentials of Human Genetics. Second Edition. Jaypee Brothers Medical Publishers (P) Ltd.



|
|
|
|
علامات بسيطة في جسدك قد تنذر بمرض "قاتل"
|
|
|
|
|
|
|
أول صور ثلاثية الأبعاد للغدة الزعترية البشرية
|
|
|
|
|
|
|
العتبة الحسينية تطلق فعاليات المخيم القرآني الثالث في جامعة البصرة
|
|
|