























النبات

مواضيع عامة في علم النبات
الجذور - السيقان - الأوراق
النباتات الوعائية واللاوعائية
البذور (مغطاة البذور - عاريات البذور)
الطحالب
النباتات الطبية
الحيوان
مواضيع عامة في علم الحيوان
علم التشريح
التنوع الإحيائي
البايلوجيا الخلوية
الأحياء المجهرية
البكتيريا
الفطريات
الطفيليات
الفايروسات
علم الأمراض
الاورام
الامراض الوراثية
الامراض المناعية
الامراض المدارية
اضطرابات الدورة الدموية
مواضيع عامة في علم الامراض
الحشرات
التقانة الإحيائية
مواضيع عامة في التقانة الإحيائية
التقنية الحيوية المكروبية
التقنية الحيوية والميكروبات
الفعاليات الحيوية
وراثة الاحياء المجهرية
تصنيف الاحياء المجهرية
الاحياء المجهرية في الطبيعة
أيض الاجهاد
التقنية الحيوية والبيئة
التقنية الحيوية والطب
التقنية الحيوية والزراعة
التقنية الحيوية والصناعة
التقنية الحيوية والطاقة
البحار والطحالب الصغيرة
عزل البروتين
هندسة الجينات
التقنية الحياتية النانوية
مفاهيم التقنية الحيوية النانوية
التراكيب النانوية والمجاهر المستخدمة في رؤيتها
تصنيع وتخليق المواد النانوية
تطبيقات التقنية النانوية والحيوية النانوية
الرقائق والمتحسسات الحيوية
المصفوفات المجهرية وحاسوب الدنا
اللقاحات
البيئة والتلوث
علم الأجنة
اعضاء التكاثر وتشكل الاعراس
الاخصاب
التشطر
العصيبة وتشكل الجسيدات
تشكل اللواحق الجنينية
تكون المعيدة وظهور الطبقات الجنينية
مقدمة لعلم الاجنة
الأحياء الجزيئي
مواضيع عامة في الاحياء الجزيئي
علم وظائف الأعضاء
الغدد
مواضيع عامة في الغدد
الغدد الصم و هرموناتها
الجسم تحت السريري
الغدة النخامية
الغدة الكظرية
الغدة التناسلية
الغدة الدرقية والجار الدرقية
الغدة البنكرياسية
الغدة الصنوبرية
مواضيع عامة في علم وظائف الاعضاء
الخلية الحيوانية
الجهاز العصبي
أعضاء الحس
الجهاز العضلي
السوائل الجسمية
الجهاز الدوري والليمف
الجهاز التنفسي
الجهاز الهضمي
الجهاز البولي
المضادات الميكروبية
مواضيع عامة في المضادات الميكروبية
مضادات البكتيريا
مضادات الفطريات
مضادات الطفيليات
مضادات الفايروسات
علم الخلية
الوراثة
الأحياء العامة
المناعة
التحليلات المرضية
الكيمياء الحيوية
مواضيع متنوعة أخرى
الانزيمات

Chronic obstructive pulmonary disease (COPD)
 المؤلف:
James Carton
المؤلف:
James Carton
 المصدر:
Oxford Handbook of Clinical Pathology 2024
المصدر:
Oxford Handbook of Clinical Pathology 2024
 الجزء والصفحة:
3rd edition , p66-67
الجزء والصفحة:
3rd edition , p66-67
 2025-01-20
2025-01-20
 954
954




+
-
20
Definition
• A chronic lung condition characterized by breathlessness due to poorly reversible and progressive airflow obstruction.
Epidemiology
• Very common disease with a prevalence of 1– 4% of the population.
• Mostly a disease of middle- aged to elderly adult smokers.
Aetiology
• 85% of cases are caused by smoking.
• Most of the remainder are attributable to previous workplace exposure to dusts and fumes.
• A very small number are related to α1-antitrypsin deficiency.
Pathogenesis
• Inflammation and scarring of small bronchioles are thought to be the main source of airflow obstruction.
• Imbalance of proteases and antiproteases causes destruction of the lung parenchyma with dilation of terminal airspaces (emphysema) and air trapping.
• Mucous gland hyperplasia and irritant effects of smoke causes productive cough (chronic bronchitis).
Presentation
• Sudden onset of exertional breathlessness on a background of prolonged cough and sputum production.
• Spirometry shows d forced expiratory volume in 1 s (FeV1) and d FeV1/ forced vital capacity (FVC) ratio (Fig. 1).
Macroscopy
• the lungs are hyperinflated with thick mucus in the airways and dilated terminal airspaces.
• Bullae may be present.
Histopathology
• Chronic inflammation and fibrosis of small bronchioles (chronic obstructive bronchiolitis).
• Finely pigmented macrophages in respiratory bronchioles (respiratory bronchiolitis).
• Dilated terminal airspaces (emphysema).
Prognosis
• Gradual decline in lung function with episodes of acute exacerbation due to infection, pneumothorax, or pulmonary embolism.
• Pulmonary hypertension and right ventricular failure then occur.
• Left ventricular failure often coexists due to ischaemic heart disease.
• Death is often related to both respiratory and cardiac failure.
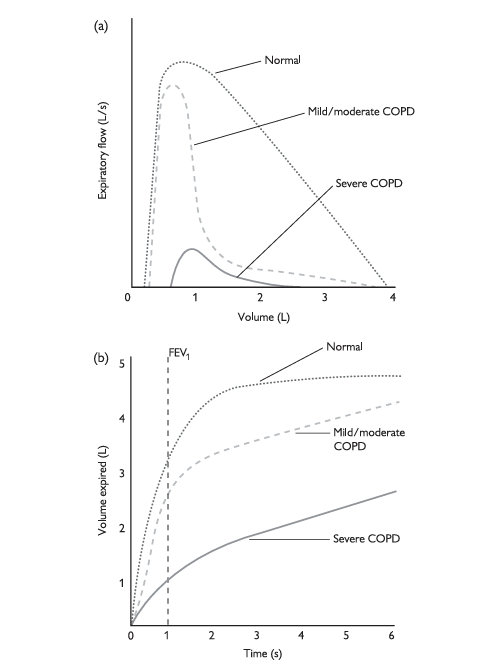
Fig.1 (a) Flow– volume loops in a normal individual, compared with patients with COPD. In mild to moderate COPD, the immediate flow is relatively normal (this is why peak flow can be normal in patients with early COPD), but then the airflow rapidly decreases. In severe COPD, the airflow is very poor with prominent air trapping (note how at the start of expiration, there is already nearly 1 L of air in the lungs). (b) Spirometry in a normal individual, compared with patients with COPD. note how in COPD, the forced expiratory volume in 1 s (FeV1) is reduced, but the final volume expired is relatively normal (they just take longer to get there!), hence the FeV1- to- FVC ratio is lowered. Reproduced with permission from Clinical Pathology (Oxford Core texts), Carton, James, Daly, Richard, and Ramani, Pramila, Oxford University Press (2006), p. 115, Figure 7.7.
 الاكثر قراءة في مواضيع عامة في علم الامراض
الاكثر قراءة في مواضيع عامة في علم الامراض
 اخر الاخبار
اخر الاخبار
اخبار العتبة العباسية المقدسة

الآخبار الصحية


مواضيع ذات صلة
 قسم الشؤون الفكرية يصدر كتاباً يوثق تاريخ السدانة في العتبة العباسية المقدسة
قسم الشؤون الفكرية يصدر كتاباً يوثق تاريخ السدانة في العتبة العباسية المقدسة "المهمة".. إصدار قصصي يوثّق القصص الفائزة في مسابقة فتوى الدفاع المقدسة للقصة القصيرة
"المهمة".. إصدار قصصي يوثّق القصص الفائزة في مسابقة فتوى الدفاع المقدسة للقصة القصيرة (نوافذ).. إصدار أدبي يوثق القصص الفائزة في مسابقة الإمام العسكري (عليه السلام)
(نوافذ).. إصدار أدبي يوثق القصص الفائزة في مسابقة الإمام العسكري (عليه السلام)



















