























النبات

مواضيع عامة في علم النبات
الجذور - السيقان - الأوراق
النباتات الوعائية واللاوعائية
البذور (مغطاة البذور - عاريات البذور)
الطحالب
النباتات الطبية
الحيوان
مواضيع عامة في علم الحيوان
علم التشريح
التنوع الإحيائي
البايلوجيا الخلوية
الأحياء المجهرية
البكتيريا
الفطريات
الطفيليات
الفايروسات
علم الأمراض
الاورام
الامراض الوراثية
الامراض المناعية
الامراض المدارية
اضطرابات الدورة الدموية
مواضيع عامة في علم الامراض
الحشرات
التقانة الإحيائية
مواضيع عامة في التقانة الإحيائية
التقنية الحيوية المكروبية
التقنية الحيوية والميكروبات
الفعاليات الحيوية
وراثة الاحياء المجهرية
تصنيف الاحياء المجهرية
الاحياء المجهرية في الطبيعة
أيض الاجهاد
التقنية الحيوية والبيئة
التقنية الحيوية والطب
التقنية الحيوية والزراعة
التقنية الحيوية والصناعة
التقنية الحيوية والطاقة
البحار والطحالب الصغيرة
عزل البروتين
هندسة الجينات
التقنية الحياتية النانوية
مفاهيم التقنية الحيوية النانوية
التراكيب النانوية والمجاهر المستخدمة في رؤيتها
تصنيع وتخليق المواد النانوية
تطبيقات التقنية النانوية والحيوية النانوية
الرقائق والمتحسسات الحيوية
المصفوفات المجهرية وحاسوب الدنا
اللقاحات
البيئة والتلوث
علم الأجنة
اعضاء التكاثر وتشكل الاعراس
الاخصاب
التشطر
العصيبة وتشكل الجسيدات
تشكل اللواحق الجنينية
تكون المعيدة وظهور الطبقات الجنينية
مقدمة لعلم الاجنة
الأحياء الجزيئي
مواضيع عامة في الاحياء الجزيئي
علم وظائف الأعضاء
الغدد
مواضيع عامة في الغدد
الغدد الصم و هرموناتها
الجسم تحت السريري
الغدة النخامية
الغدة الكظرية
الغدة التناسلية
الغدة الدرقية والجار الدرقية
الغدة البنكرياسية
الغدة الصنوبرية
مواضيع عامة في علم وظائف الاعضاء
الخلية الحيوانية
الجهاز العصبي
أعضاء الحس
الجهاز العضلي
السوائل الجسمية
الجهاز الدوري والليمف
الجهاز التنفسي
الجهاز الهضمي
الجهاز البولي
المضادات الميكروبية
مواضيع عامة في المضادات الميكروبية
مضادات البكتيريا
مضادات الفطريات
مضادات الطفيليات
مضادات الفايروسات
علم الخلية
الوراثة
الأحياء العامة
المناعة
التحليلات المرضية
الكيمياء الحيوية
مواضيع متنوعة أخرى
الانزيمات

Protein-energy (calorie) malnutrition
 المؤلف:
Denise R. Ferrier
المؤلف:
Denise R. Ferrier
 المصدر:
Lippincott Illustrated Reviews: Biochemistry
المصدر:
Lippincott Illustrated Reviews: Biochemistry
 الجزء والصفحة:
الجزء والصفحة:
 7-12-2021
7-12-2021
 2152
2152




+
-
20
Protein-energy (calorie) malnutrition
In developed countries, protein-energy malnutrition (PEM), also known as protein-energy undernutrition (PEU), is most commonly seen in patients with medical conditions that decrease appetite or alter how nutrients are digested or absorbed or in hospitalized patients with major trauma or infections. [Note: Such highly catabolic patients frequently require intravenous (IV, or parenteral) or tube-based (enteral) administration of nutrients.] PEM may also be seen in children or the elderly who are malnourished. In developing countries, an inadequate intake of protein and/or calories is the primary cause of PEM. Affected individuals show a variety of symptoms, including a depressed immune system with a reduced ability to resist infection. Death from secondary infection is common. PEM is a spectrum of degrees of malnutrition, and two extreme forms are kwashiorkor and marasmus (Fig. 1). [Note: Marasmic kwashiorkor has features of both forms.]

Figure 1: Physical features of extreme protein-energy malnutrition (PEM) in
children. [Note: The fatty liver and skin and hair changes of kwashiorkor are not
seen in marasmus.]
1. Kwashiorkor: Kwashiorkor occurs when protein deprivation is relatively greater than the reduction in total calories. Protein deprivation is associated with severely decreased synthesis of visceral protein.
Kwashiorkor is commonly seen in developing countries in children after weaning at about age 1 year, when their diet consists predominantly of carbohydrates. Typical symptoms include stunted growth, skin lesions, depigmented hair, anorexia, fatty liver, bilateral pitting edema, and decreased serum albumin concentration. Edema results from the lack of adequate blood proteins, primarily albumin, to maintain the distribution of water between blood and tissues. It may mask muscle and fat loss.
Therefore, chronic malnutrition is reflected in the level of serum albumin. [Note: Because caloric intake from carbohydrates may be adequate, insulin levels suppress lipolysis and proteolysis. Kwashiorkor is, therefore, nonadapted malnutrition.]
2. Marasmus: Marasmus occurs when calorie deprivation is relatively greater than the reduction in protein. It usually occurs in developing countries in children younger than age 1 year when breast milk is supplemented or replaced with watery gruels of native cereals that are usually deficient in both protein and calories. Typical symptoms include arrested growth, extreme muscle wasting and depletion of subcutaneous fat (emaciation), weakness, and anemia (Fig. 2). Individuals with marasmus do not show the edema observed in kwashiorkor. [Note: Refeeding severely malnourished individuals can result in hypophosphatemia , because any available phosphate is used
to phosphorylate carbohydrate intermediates. Milk is frequently given
because it is rich in phosphate.]
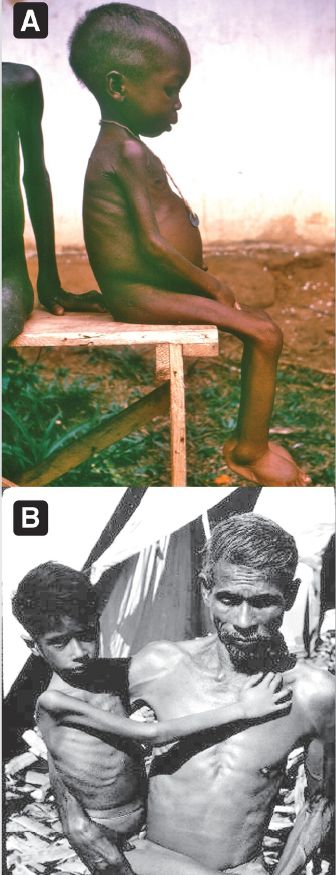
Figure 2: A. Listless child with kwashiorkor. Note the swollen belly and lower legs. B. Child suffering with marasmus.
Cachexia, a wasting disorder characterized by loss of appetite and muscle atrophy (with or without increased lipolysis) that cannot be reversed by conventional nutritional support, is seen with a number of chronic diseases, such as cancer and chronic pulmonary and renal disease. It is associated with decreased treatment tolerance and response and decreased survival time.
 الاكثر قراءة في الكيمياء الحيوية
الاكثر قراءة في الكيمياء الحيوية
 اخر الاخبار
اخر الاخبار
اخبار العتبة العباسية المقدسة

الآخبار الصحية


مواضيع ذات صلة
 قسم الشؤون الفكرية يصدر كتاباً يوثق تاريخ السدانة في العتبة العباسية المقدسة
قسم الشؤون الفكرية يصدر كتاباً يوثق تاريخ السدانة في العتبة العباسية المقدسة "المهمة".. إصدار قصصي يوثّق القصص الفائزة في مسابقة فتوى الدفاع المقدسة للقصة القصيرة
"المهمة".. إصدار قصصي يوثّق القصص الفائزة في مسابقة فتوى الدفاع المقدسة للقصة القصيرة (نوافذ).. إصدار أدبي يوثق القصص الفائزة في مسابقة الإمام العسكري (عليه السلام)
(نوافذ).. إصدار أدبي يوثق القصص الفائزة في مسابقة الإمام العسكري (عليه السلام)



















